Ling Chen, Ting Ma, Liang Wang, Lixin Wang, Minmin Li, Rong Zhu. Unilateral pleural effusion secondary to Takayasu arteritis: a case report and literature review[J]. The Journal of Biomedical Research, 2022, 36(2): 141-144. DOI: 10.7555/JBR.36.20210190
Citation:
Ling Chen, Ting Ma, Liang Wang, Lixin Wang, Minmin Li, Rong Zhu. Unilateral pleural effusion secondary to Takayasu arteritis: a case report and literature review[J]. The Journal of Biomedical Research, 2022, 36(2): 141-144. DOI: 10.7555/JBR.36.20210190
Ling Chen, Ting Ma, Liang Wang, Lixin Wang, Minmin Li, Rong Zhu. Unilateral pleural effusion secondary to Takayasu arteritis: a case report and literature review[J]. The Journal of Biomedical Research, 2022, 36(2): 141-144. DOI: 10.7555/JBR.36.20210190
Citation:
Ling Chen, Ting Ma, Liang Wang, Lixin Wang, Minmin Li, Rong Zhu. Unilateral pleural effusion secondary to Takayasu arteritis: a case report and literature review[J]. The Journal of Biomedical Research, 2022, 36(2): 141-144. DOI: 10.7555/JBR.36.20210190
Rong Zhu, The Huai'an Clinical College of Xuzhou Medical University, 6 Beijing West Road, Huaiyin District, Huai'an City, Jiangsu Province 223300, China. E-mail: lszhurong@163.com
Takayasu arteritis (TA) is a chronic, nonspecific inflammatory disease of large and medium-sized vessels that primarily involves the aorta and its branches. TA involving the pulmonary arteries has a prevalence ranging from 14% to 86%, which can lead to pulmonary hypertension, a progressive increase in pulmonary artery pressure, and eventually death from right heart failure. The presentation of pulmonary arteritis (PA) is very nonspecific, with a reported misdiagnosis rate of up to 60% and a diagnosis time ranging from 1 month to more than 10 years. The clinical manifestation of pleural effusion is very rare in both TA and PA cases. Based on our literature review, this is the 6th reported case of TA with pleural effusion, and the specific mechanism of TA with pleural effusion is still unclear. The characteristics of this case and the previously reported cases are summarized in this article to improve the understanding of TA and PA and reduce the misdiagnosis rate.
Takayasu arteritis (TA) is a type of nonspecific chronic large vessel vasculitis characterized by granulomatous inflammation in the vessel wall of the aorta and its major branches[1]. The pathophysiological progression of full-thickness inflammation of the vessel wall and the subsequent fibrosis usually occurs with vascular stenosis and/or occlusion, causing ischemia of the corresponding organs, which is associated with a high mortality[2]. The involvement of pulmonary artery is not rare in patients with TA[3–4]. Patients with pulmonary artery involvement commonly present with respiratory symptoms[5] , with rare reports of pleural effusion. Herein, we report a case of unilateral pleural effusion as the main manifestation to improve clinicians' understanding of TA.
The case report was approved by the Ethics Committee of Huai'an First People's Hospital (Ethics approval No. YX-2021-056-01).
Case report
A 49-year-old female was admitted to our hospital in May 2020 due to cough and expectoration (mainly white sticky sputum) with chest pain of no obvious cause for four months. The efficacy of anti-infective therapy in local hospitals was poor. Blood routine examination before admission showed moderate anemia. Chest CT showed a large amount of pleural effusion on the right side, main pulmonary artery dilation with enlarged left hilum, and right-side pneumonia. The patient had a history of anemia for more than 20 years without receiving standardized treatment. Physical examination: T, 36.2 °C; P, 98/minute; R, 20/minute; BP, 100/55 mmHg. The respiratory movement of the right lower lung was weakened. Tremor was weakened. There was percussion dullness. Breath sound was low, and no wet and dry rales were heard.
Laboratory and imaging examinations
The patient's laboratory and imaging test results are as follows. Inflammatory biomarkers: C-reactive protein, 26.2 mg/L; erythrocyte sedimentation rate, 61 mm/h; white blood cell, 4.74×109/L; D2 polymer, 3.25 mg/L; hemoglobin, 73 g/L. Ultrasound of the thorax and abdomen: right pleural effusion (upper and lower diameter approximately 6.3 cm, depth about 10.2 cm); splenomegaly; N-terminal pro-B-type natriuretic peptide, procalcitonin, antineutrophil cytoplasmic antibody. T-SPOT.TB, tumor indicators, liver and kidney function panel tests, myocardial enzyme, stool and urine tests were all normal. The test of the closed chest drainage fluid at admission suggest an exudative pleural effusion with a moderate CEA level, and the proliferation of mesothelioid cells and lymphocytes were observed under the microscope. Echocardiography revealed moderate to severe pulmonary hypertension. CTA examination of the pulmonary arteries showed multiple thickening of the walls of the aorta, mild-to-severe lumen stenosis and arteritis of the right pulmonary, common carotid, subclavian arteries; the pulmonary artery in the middle and upper lobes of the right lung was not visualized; a small amount of fluid in the pericardial cavity and a moderate amount of fluid in the right thoracic cavity were observed (Fig. 1). The completion of an ultrasound examination of the circumferential vessels showed bilateral common carotid artery and bilateral subclavian artery stenosis (50% to 69%) and innominate artery stenosis (less than 50%).
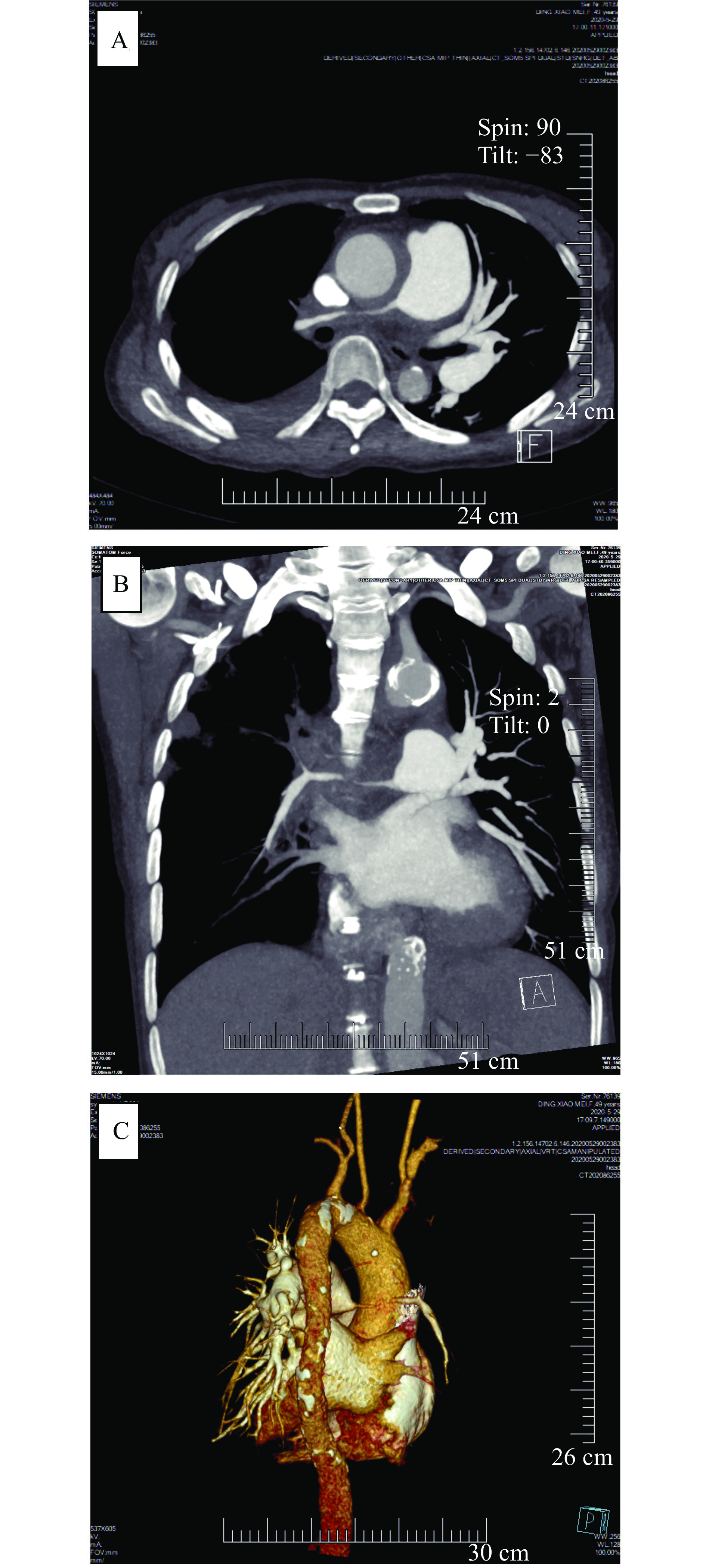
Figure
1.CTPA.
A and B: CT coronal and axial scans showed severe stenosis of the right pulmonary artery trunk and its branches, and strips of low-density filling defects were seen in the wall. C: The right pulmonary artery trunk and its branches were severely stenosed with a ductal diameter of approximately 5 mm.
The main manifestations of this patient were cough, expectoration, and chest pain. Echocardiography showed pulmonary hypertension. Pulmonary artery CTA and vascular ultrasound examination showed pulmonary artery and systemic vascular stenosis and occlusion, excluding congenital artery stenosis, atherosclerosis, thromboangiitis obliterans, Behcet's disease and nodular polyarteritis, and the diagnosis of TA was made. Methylprednisolone (40 mg, orally) and cyclophosphamide (0.4 g, intravenously) were administered for treatment. After being discharged from the hospital, the patient was followed up every month to receive 0.4 g cyclophosphamide intravenously and have her glucocorticoid dosage adjusted. The patient had no symptoms of cough, sputum, or chest pain, and the pleural effusion disappeared half a year later. One and a half years later, her hemoglobin level was 120 g/L.
Discussion
The etiology of TA is thought to be related to genetics[6], endocrine abnormalities, immune dysfunction, and cytokine inflammation after infection (Streptococcus, Mycobacterium tuberculosis, virus, etc.)[7]. The clinical symptoms of TA are generally nonspecific and vary depending on the affected vessels[8] and the severity of the disease[4]. The diagnosis of TA mainly relies on clinical and imaging findings showing the pathological changes[9]: wall thickening, thrombus formation, stenotic and occlusive lesions due to inflammation and endothelial damage, as well as destruction of the muscularis and elastic layers caused by dilatation and aneurysms[7]. Glucocorticoids (GC), as a first line treatment, is the most effective drug for TA[9]. As experience has shown that the cumulative GC demand in TA is high, GC-sparing treatment with moderately potent immunosuppressants, such as methotrexate, azathioprine, and mycophenolate mofetil, is recommended to TA patient from the time of initial diagnosis[10].
The incidence of pulmonary arteritis (PA) in patients with TA varies greatly among studies (14% to 86%)[11]. Approximately, half of PA patients suffer from overt pulmonary hypertension (PH) during their disease course, mostly secondary to pulmonary artery stenosis or occlusion[4,12]. The CTA results of this patient showed lesions of varying degrees in the aorta, pulmonary, common carotid, and subclavian arteries, and the pulmonary artery in the middle and upper lobes of the right lung was invisible. Also, echocardiography indicated a moderate to severe pulmonary hypertension, so PA was considered.
Unlike conventional TA, PA is mainly characterized by respiratory symptoms[5]: dyspnea (68% to 83%), cough (20% to 66.7%), hemoptysis (20% to 57%), and chest pain (17% to 48%)[5,12–13]. Our patient had cough and chest pain, which is consistent with previous reports, but she also had a large unilateral pleural effusion. Using "Takayasu arteritis" and "pleural effusion" as keywords, we retrieved 5 related papers in the Wanfang, CNKI, and PubMed databases, and compiled the data of the 5 patients reported in the literature (Table 1)[14–18]. Combining the data from both literature and this case, it can be summarized that TA with pleural effusion is more frequent in women and has a fairly large age span. The patients under 45 years of age may have fever and be easily misdiagnosed as tuberculosis, while those over 45 years of age tend to have pulmonary artery involvement and present with respiratory and chest pain manifestations. The most commonly involved artery is the subclavian artery, which may be vasodilated proximally. The most common site is the left side, and the nature is exudative, ranging from small to large amounts. Unilateral pleural effusion may be related to pleural irritation due to pathological changes in the vessels anatomically proximal to the large arteries on the left side of the thorax[16–17].
Table
1.
Data of five TA patients with unilateral pleural effusion
Left; Exudative; Small amount; Recurring with disease activity
Left; Exudative
Left; Small amount; Exudative
Left; Massive; Bloody
Left; Massive; Exudative
Involved narrowed or occluded arteries
Subclavicul bilaterally
Right subclavian; Left coronary artery
Proximal aorta; Right carotid
Subclavicul bilaterally; Right upper pulmonary
Upper and lower left pulmonary artery
Treatment
Misdiagnosed as tuberculosis, pleural effusion recurring along with irregular corticosteroids application, and after TA diagnosis, corticosteroids given again.
Prednisolone 60 mg daily with methotrexate 2.5 mg weekly increasing the dose to 7.5 mg weekly a month.
Prednisone 50 mg/day and methotrexate 7.5 mg/week tapered over months to 5 mg/day prednisone and aspirin.
Methylprednisolone 80 mg, 1 time/8 hours, IV, gradually reduced to prednisone 20 mg, 2 times/day orally, cyclophosphamide 0.4 g IV, with torasemide and other symptomatic supportive treatment.
Methylprednisolone 40 mg qd×7 days, intravenous drip, gradually reduced to prednisone acetate tablets 30 m/day orally and hydroxychloroquine sulfate 0.2 g bid.
Hb: hemoglobin; CRP: C-reactive protein; ESR: erythrocyte sedimentation rate; IV: intravenous; qd: once a day; bid: twice a day.
The production of pleural fluid comes mainly from the filtration of the wall pleura capillaries, while the absorption of pleural fluid depends on the reabsorption of the pleura wall (under normal conditions, the role of the dirty pleura in the circulation of pleural fluid is smaller)[19]. Pleural fluid production and absorption are normally in a dynamic equilibrium, and when disturbed in some pathological conditions, pleural effusion is formed. The etiology of pleural effusion varies, and in general, the first step in diagnosis is to determine whether the nature of the effusion is transudative or exudative. Exudative pleural effusions are usually prioritized as pneumonia, tuberculosis, or malignancy[20]. When looking for causes, we often focus on common causes and miss rare or uncommon causes. In this paper, we report a rare clinical presentation (unilateral pleural effusion) of a rare disease (i.e., TA), and review the relevant literature to summarize the general characteristics of such a disease, hoping to improve clinicians' knowledge and understanding of TA and pleural effusion. However, because there are few relevant reports, the etiology and specific pathogenesis cannot be clarified, and more clinical data and research support are needed.
Watts RA, Hatemi G, Burns JC, et al. Global epidemiology of vasculitis[J]. Nat Rev Rheumatol, 2022, 18(1): 22–34. doi: 10.1038/s41584-021-00718-8
[2]
Alnabwani D, Patel P, Kata P, et al. The epidemiology and clinical manifestations of Takayasu arteritis: a descriptive study of case reports[J]. Cureus, 2021, 13(9): e17998. doi: 10.7759/cureus.17998
Jiang X, Zhu Y, Zhou Y, et al. Clinical features and survival in Takayasu's arteritis-associated pulmonary hypertension: a nationwide study[J]. Eur Heart J, 2021, 42(42): 4298–4305. doi: 10.1093/eurheartj/ehab599
[5]
Lin J, Zhang T, Peng M, et al. Clinical features of pulmonary artery involvement in Takayasu's arteritis and recent advances[J]. Chin J Tuberc Respir Dis, 2021, 44(1): 54–59. doi: 10.3760/cma.j.cn112147-20200316-00349
[6]
Villon MLFZ, De La Rocha JAL, Espinoza LR. Takayasu arteritis: recent developments[J]. Curr Rheumatol Rep, 2019, 21(9): 45. doi: 10.1007/s11926-019-0848-3
[7]
Russo RAG, Katsicas MM. Takayasu arteritis[J]. Front Pediatr, 2018, 6: 265. doi: 10.3389/fped.2018.00265
Hellmich B. Treatment of Takayasu arteritis[J]. Z Rheumatol (in German), 2020, 79(6): 532–544. doi: 10.1007/s00393-020-00806-2.
[11]
Dou J, Gong J, Ma Z, et al. The analysis of the clinical records diagnosed as Takayasu's arteritis with pulmonary vascular involvement[J]. Chin J Tuberc Respir Dis, 2016, 39(8): 603–607. doi: 10.3760/cma.j.issn.1001-0939.2016.08.011
[12]
Yang J, Peng M, Shi J, et al. Pulmonary artery involvement in Takayasu's arteritis: diagnosis before pulmonary hypertension[J]. BMC Pulm Med, 2019, 19(1): 225. doi: 10.1186/s12890-019-0983-7
[13]
He Y, Lv N, Dang A, et al. Pulmonary artery involvement in patients with Takayasu arteritis[J]. J Rheumatol, 2020, 47(2): 264–272. doi: 10.3899/jrheum.190045
[14]
Kawai T, Yamada Y, Tsuneda J, et al. Pleural effusion associated with aortitis syndrome[J]. Chest, 1975, 68(6): 826–828. doi: 10.1378/chest.68.6.826
[15]
Achari V, Prakash S. Takayasu's disease presenting with pain chest, prolonged pyrexia and pleural effusion[J]. J Assoc Physicians India, 2005, 53: 722–724. https://pubmed.ncbi.nlm.nih.gov/16398084/
[16]
Schattner A, Klepfish A. Left pleural effusion and fever of unknown origin-a clue to thoracic arterial pathology[J]. J Gen Intern Med, 2012, 27(8): 1084–1087. doi: 10.1007/s11606-012-2008-6
[17]
Gui X, Cao M, Liu Y, et al. Unilateral pleural effusion as first manifestation in Takayasu arteritis: a case report and review of literature[J]. Chin J Tuberc Respir Dis, 2016, 39(10): 768–772. doi: 10.3760/cma.j.issn.1001-0939.2016.10.006
[18]
Liang Y, Zuo Q, Wang T. A case of Takayasu's arteritis with unilateral pleural effusion as the main manifestation and literature review[J]. Acta Univ Med Nanjing (Nat Sci) (in Chinese), 2018, 38(2): 266–268. doi: 10.7655/NYDXBNS20180228.
[19]
Light MD, Richard W. Plural disease[M]. 6th ed. Philadelphia: Lippincott Williams & Wilkins, 2013: 128–129.
[20]
Na MJ. Diagnostic tools of pleural effusion[J]. Tuberc Respir Dis, 2014, 76(5): 199–210. doi: 10.4046/trd.2014.76.5.199
Left; Exudative; Small amount; Recurring with disease activity
Left; Exudative
Left; Small amount; Exudative
Left; Massive; Bloody
Left; Massive; Exudative
Involved narrowed or occluded arteries
Subclavicul bilaterally
Right subclavian; Left coronary artery
Proximal aorta; Right carotid
Subclavicul bilaterally; Right upper pulmonary
Upper and lower left pulmonary artery
Treatment
Misdiagnosed as tuberculosis, pleural effusion recurring along with irregular corticosteroids application, and after TA diagnosis, corticosteroids given again.
Prednisolone 60 mg daily with methotrexate 2.5 mg weekly increasing the dose to 7.5 mg weekly a month.
Prednisone 50 mg/day and methotrexate 7.5 mg/week tapered over months to 5 mg/day prednisone and aspirin.
Methylprednisolone 80 mg, 1 time/8 hours, IV, gradually reduced to prednisone 20 mg, 2 times/day orally, cyclophosphamide 0.4 g IV, with torasemide and other symptomatic supportive treatment.
Methylprednisolone 40 mg qd×7 days, intravenous drip, gradually reduced to prednisone acetate tablets 30 m/day orally and hydroxychloroquine sulfate 0.2 g bid.
Hb: hemoglobin; CRP: C-reactive protein; ESR: erythrocyte sedimentation rate; IV: intravenous; qd: once a day; bid: twice a day.
 Authors and Reviewers
Authors and Reviewers

 DownLoad:
DownLoad:

