Xu Ke, Huo Xiang, Zu Rongqiang, Wang Shenjiao, Qin Yuanfang, Dai Qigang, Qi Xian, Yu Huiyan, Chen Lilin, Hong Lei, Xu Yangting, Yi Qianhua, Wang Weixiang, Wang Xuan, Dai Wenjun, Zha Jie, Han Weining, Bao Changjun. Etiological characteristics of influenza-like illness in Jiangsu province from 2012 to 2016[J]. The Journal of Biomedical Research, 2019, 33(6): 398-407. DOI: 10.7555/JBR.33.20180128
Citation:
Xu Ke, Huo Xiang, Zu Rongqiang, Wang Shenjiao, Qin Yuanfang, Dai Qigang, Qi Xian, Yu Huiyan, Chen Lilin, Hong Lei, Xu Yangting, Yi Qianhua, Wang Weixiang, Wang Xuan, Dai Wenjun, Zha Jie, Han Weining, Bao Changjun. Etiological characteristics of influenza-like illness in Jiangsu province from 2012 to 2016[J]. The Journal of Biomedical Research, 2019, 33(6): 398-407. DOI: 10.7555/JBR.33.20180128
Xu Ke, Huo Xiang, Zu Rongqiang, Wang Shenjiao, Qin Yuanfang, Dai Qigang, Qi Xian, Yu Huiyan, Chen Lilin, Hong Lei, Xu Yangting, Yi Qianhua, Wang Weixiang, Wang Xuan, Dai Wenjun, Zha Jie, Han Weining, Bao Changjun. Etiological characteristics of influenza-like illness in Jiangsu province from 2012 to 2016[J]. The Journal of Biomedical Research, 2019, 33(6): 398-407. DOI: 10.7555/JBR.33.20180128
Citation:
Xu Ke, Huo Xiang, Zu Rongqiang, Wang Shenjiao, Qin Yuanfang, Dai Qigang, Qi Xian, Yu Huiyan, Chen Lilin, Hong Lei, Xu Yangting, Yi Qianhua, Wang Weixiang, Wang Xuan, Dai Wenjun, Zha Jie, Han Weining, Bao Changjun. Etiological characteristics of influenza-like illness in Jiangsu province from 2012 to 2016[J]. The Journal of Biomedical Research, 2019, 33(6): 398-407. DOI: 10.7555/JBR.33.20180128
Department of Acute Infectious Disease Control and Prevention, Jiangsu Provincial Center for Disease Control and Prevention, Nanjing, Jiangsu 210009, China
2.
Department of Acute Infectious Disease Control and Prevention, Suzhou Municipal Center for Disease Control and Prevention, Suzhou, Jiangsu 215004, China
3.
Department of Acute Infectious Disease Control and Prevention, Nanjing Municipal Center for Disease Control and Prevention, Nanjing, Jiangsu 210003, China
4.
Department of Acute Infectious Disease Control and Prevention, Taizhou Municipal Center for Disease Control and Prevention, Taizhou, Jiangsu 225300, China
Funds: This is an open access article under the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited.
Changjun Bao, Department of Acute Infectious Disease Control and Prevention, Jiangsu Provincial Center for Disease Control and Prevention, Nanjing, Jiangsu 210009, China. Tel: +86-25-83759404, E-mail: bao2000_cn@163.com
Influenza-like illness (ILI) is an acute respiratory infection caused by various pathogens. However, the epidemiologic characteristics of ILI pathogens in Jiangsu province are unclear. To better understand the ILI etiology, the characteristics of the pathogens from nasopharyngeal swab samples of patients with ILI collected from 2012 to 2016 in 6 hospitals in Jiangsu province were studied. The pathogens, including influenza virus, respiratory syncytial virus (RSV), rhinovirus (HRV), adenovirus (ADV), herpes simplex virus (HSV), human coronavirus (hCoV), Streptococcus pneumoniae and Haemophilus influenzae, were detected by real-time PCR. At least one pathogen was identified in 1 334 of the patients (40.23%). Among viruses, HRV, influenza A virus (Flu A), ADV and RSV were the most frequently detected. ADV was the only pathogen that was distributed evenly in different years and regions (P>0.05). The etiological distribution varied in different age groups. Streptococcus pneumoniae was the most common pathogen in co-infections with a co-detection rate of 64.57% (319/494). The spectrum of etiologies could help to estimate disease burden and provide guidance for vaccination.
Acute respiratory infections are common illnesses with a high morbidity in young children in developing countries and in the elderly globally[1–2]. Influenza-like illness (ILI) is one of the acute respiratory infections, defined by a fever higher than or equal to 38 °C accompanied by a cough[3]. China has been one of the Global Influenza Surveillance and Response System (GISRS) National Influenza Centers for decades. ILI surveillance has been performed in Jiangsu province for 15 years. During these years, the epidemiology of influenza has been studied. However, pathogens responsible for many ILI cases, if not influenza viruses, needed to be further defined. These pathogens can not only cause ILI[4– 6], but also have great potential to cause severe respiratory diseases such as croup, bronchiolitis, and pneumonia, which often require hospitalization, especially in very young and elderly individuals with underlying chronic conditions[7].
Previous studies have showed that Streptococcus pneumoniae (S. pneumoniae) and Haemophilus influenzae (H. influenzae) are the most common bacteria responsible for respiratory infections[8]. Common respiratory viruses, including respiratory syncytial virus (RSV), rhinovirus (HRV), adenovirus (ADV), herpes simplex virus (HSV), human coronaviruses (HCoV-OC43 and HCoV-229E) are also indicated as causative agents of respiratory infections in some reports[9– 11]. In addition, over the past decade, a number of new viruses have been reported, including hCoV-NL63 and hCoV-HKU1[12–15]. Microorganisms causing ILI are complex and diverse, varying by region and season. Moreover, acute respiratory tract disease in humans sometimes presents with co-infection by more than one organism[16–17].
The pathogenic spectrum of ILI in Jiangsu province has not been well characterized to date. Much less is known about the epidemiologic characteristics of the ILI pathogens. Therefore, the aim of this study was to investigate the prevalence and the epidemiologic characteristics of different pathogens causing ILI in Jiangsu province in China from 2012 to 2016.
Materials and methods
Ethics statement
This project was part of public health surveillance in Jiangsu province. Verbal consent during the outpatient visit was obtained from each participant or from his or her parent/guardian. The study protocol was approved by the Ethics Committee of the Jiangsu Provincial Center for Disease Control and Prevention, and the study was conducted in compliance with the principles of the Declaration of Helsinki.
Surveillance location
Jiangsu province is a densely populated province in China, with an area of 107 200 km2. At the end of 2017, its population has reached 80.293 million, with males accounting for 50.33% with mainly Han ethnicity (99.5%). The age of the population consisted of 10.94 million aged 0–14, 58.857 million aged 15–64, and 10.732 million aged 65 and over.
The surveillance for ILI started in 2012 and was located in 6 sentinel hospitals of three cities (Nanjing, Taizhou and Suzhou) of Jiangsu province, China. The sentinel sites were chosen with careful consideration of geographical representation and surveillance capability. Of the six sentinel hospitals two are children's hospitals, two adult hospitals, and two hospitals for both adults and children (Supplementary Fig. 1, available online). The selected hospitals were among the largest hospitals in the country and served mainly the local population. National surveillance of ILI has been performed for many years in these sentinel sites. Furthermore, their capacities for laboratory testing in disease control and prevention were qualified annually by the National Influenza Center.
Definition of ILI and patient enrollment
ILI was defined as the onset of a fever, with axillary temperature ≥38 °C and following one or both of the symptoms: cough and pharyngeal discomfort. The study group consisted of outpatients from the above-mentioned 6 hospitals who met the ILI criteria with an onset less than 3 days. Nasopharyngeal swab specimens were collected from them 2 or more days a week in each sentinel hospital.
Sample collection
After the collection samples were immediately added to 3.0 mL of viral transport medium (VTM, Dulbecco's Modified Eagle Medium with 100 U/mL penicillin, 100 mg/mL streptomycin, and 2 000 U/mL amphotericin B) and stored at 4 –8 °C at the local hospital. Within 48 hours, samples were transferred on ice to a network laboratory for diagnostic testing. At the laboratory, specimens in VTM should be stored at −70 °C until further processing, if testing was not performed within 48 hours after collection.
Real-time PCR for detection
From 2012 to 2016, ten samples were selected randomly in every sentinel hospital per month. Each sample was tested simultaneously for the following pathogens: influenza A virus (Flu A), influenza B virus (Flu B), influenza C virus (Flu C), HRV, RSV, ADV, 4 strains of hCoV (hCoV-229E, hCoV-OC43, hCoV-NL63 and hCoV-HKU1), HSV, S. pneumoniae, and H. influenzae.
Nucleic acids were extracted using commercial kits (QIAmp Mini Elute Virus Spin kit, QIAamp Viral RNA Mini kit or RNeasy Mini kit, Qiagen, Valencia, CA,USA). Real-time PCR was performed to detect ADV, hCoVs, HSV, S. pneumoniae, and H. influenza, real-time RT-PCR was performed to detect the other viral agents using recommended commercial kits (Fluorescent PCR Diagnostic kits, Shanghai ZJ Bio-Tech Co., Ltd, Shanghai, China) according to the manufacturers' protocols. Positive and negative controls were included in each PCR run to test for cross contamination. Specimens with only a single pathogen detected were considered mono-infection, and those with two or more pathogens detected were regarded as co-infection.
Statistical analysis
The R project was used for all analyses (version 3.3.3). The Chi-square test was used to compare differences in the distribution of categorical variables, and Fisher's exact test was used wherever appropriate. The Mann-Whitney test was used to compare the age difference between two independent groups. All tests were two-tailed, and P<0.05 was considered statistically significant. The detection rates of all pathogens were standardized according to age groups. Seasonal index was calculated to describe the seasonal distribution of pathogens detected greater than 2%.
Results
Characteristics of outpatients with ILI
A total of 3 316 patients ranged in age from 30 days to 89 years [median, 5 years (IQR 1–31)] were enrolled in this 5-year study program (Supplementary Table 1, available online). Among them, 1 734 were male (52.29%), 1 670 were children ≤5 years of age (50.36%), and 109 were elderly individuals ≥65 years of age (3.29%). Of the 3 316 patients, 49.35% had cough and 76.11% had angina or congestion of the throat.
Spectrum of pathogenic agents
At least one of the pathogens was identified in 1 334 patients (40.23%), with a single pathogen in 915 patients (27.59%) and multiple pathogens in 419 patients (12.64%). Among all samples, 937 (28.26%) tested positive for at least one viral species, and 714 (21.53%) tested positive for at least one bacterial species.
Of the 1 334 patients confirmed with at least one etiology, the most frequently detected virus was HRV in 211 patients (6.36%), followed by Flu A in 209 patients (6.30%), ADV in 140 patients (4.22%), RSV in 133 patients (4.01%), HSV in 98 patients (2.95%), Flu B in 84 patients (2.53%), hCoV-NL63 in 61 patients (1.83%), hCoV-OC43 in 47 patients (1.42%), Flu C in 14 patients (0.42%), hCoV-229E in 14 patients (0.42%), and hCoV-HKU1 in 13 patients (0.39%). S. pneumoniae and H. influenzae were detected in 494 (14.90%) and 347 patients (10.46%), respectively.
Etiologic distribution in patients of different genders and ages
Etiologic distribution was assessed among different age groups. Flu A was the most common pathogen in children aged 6 –9 years (8.91%) and in older individuals aged 50–64 years (8.85%). HRV and RSV were detected more frequently in infants younger than 6 months of age (13.04% and 8.70%, respectively). Flu B and ADV were detected most frequently in students aged 6 –9 years. Interestingly, 4 strains of hCoV were not detected in teenagers 10–14 years of age, while HSV had the highest detection rate in this group (Table 1).
Table
1.
Characteristics of ILI patients positive at least one pathogen and the distribution at different age groups among 3 316 patients with ILI
Characteristics
Flu A
Flu B
Flu C
RSV
ADV
HRV
hCoV-229E
hCoV-OC43
hCoV-NL63
hCoV-HKU1
HSV
S. pneumoniae
H. influenzae
Male [n (%)] (n=1734)
110 (6.34)
47 (2.71)
6 (0.35)
72 (4.15)
77 (4.44)
109 (6.29)
10 (0.57)
21 (1.21)
33 (1.90)
2 (0.12)
46 (2.65)
268 (15.46)
189 (10.90)
Female [n (%)] (n=1582)
99 (6.26)
37 (2.34)
7 (0.44)
61 (3.86)
63 (3.98)
102 (6.45)
4 (0.25)
26 (1.64)
28 (1.77)
11 (0.70)
52 (3.29)
226 (14.29)
158 (9.99)
Age*(Median) (IQR)
7 (3−43)
7 (4−27)
4.5 (3−34)
2 (1−4)
3 (2−6)
3 (1.3−7)
4 (1−35)
4 (1−19)
3 (1−6)
1 (1−2)
5 (2−25)
1 (1.5−6)
6 (2−28)
<6 months [n (%)] (n=69)
3 (4.35)
0 (0.00)
1 (1.45)
6 (8.70)
2 (2.90)
9 (13.04)
1 (1.45)
2 (2.90)
1 (1.45)
0 (0.00)
2 (2.90)
16 (23.18)
2 (2.90)
6−11 months [n (%)] (n=169)
5 (2.96)
1 (0.59)
0 (0.00)
13 (7.69)
8 (4.73)
16 (9.47)
0 (0.00)
3 (1.77)
3 (1.77)
1 (0.59)
2 (1.18)
32 (18.93)
15 (8.87)
12−35 months [n (%)] (n=717)
33 (4.60)
10 (1.39)
1 (0.14)
54 (7.53)
49 (6.83)
65 (9.06)
5 (0.70)
11 (1.53)
24 (3.35)
8 (1.12)
22 (3.07)
139 (19.38)
80 (11.16)
3−5 years [n (%)] (n=715)
57 (7.97)
16 (2.24)
5 (0.70)
44 (6.15)
38 (5.31)
54 (7.55)
1 (0.14)
15 (2.10)
14 (1.96)
2 (0.28)
25 (3.50)
172 (24.05)
72 (10.07)
6−9 years [n (%)] (n=247)
22 (8.91)
26 (10.53)
0 (0.00)
5 (2.02)
20 (8.10)
21 (8.50)
0 (0.00)
2 (0.81)
4 (1.62)
0 (0.00)
9 (3.64)
46 (18.62)
37 (14.98)
10−14 years [n (%)] (n=75)
5 (6.67)
5 (6.67)
0 (0.00)
2 (2.67)
5 (6.67)
5 (6.67)
0 (0.00)
0 (0.00)
0 (0.00)
0 (0.00)
4 (5.33)
12 (16.00)
7 (9.33)
15−49 years [n (%)] (n=1 023)
62 (6.06)
19 (1.86)
6 (0.59)
5 (0.49)
17 (1.6)
34 (3.32)
4 (0.39)
13 (1.27)
13 (1.27)
1 (0.10)
26 (2.54)
63 (6.16)
110 (10.75)
50−64years) [n (%)] (n=192)
17 (8.85)
6 (3.13)
0 (0.00)
1 (0.52)
0 (0.00)
6 (3.13)
2 (1.04)
0 (0.00)
1 (0.52)
1 (0.52)
3 (1.56)
8 (4.17)
14 (7.29)
≥65 years [n (%)] (n=109)
5 (4.59)
1 (0.92)
0 (0.00)
3 (2.75)
1 (0.92)
1 (0.92)
1 (0.92)
1 (0.92)
1 (0.92)
0 (0.00)
5 (4.59)
6 (5.50)
10 (9.17)
Tatol [n (%)] (n=3 316)
209 (6.30)
84 (2.53)
13 (0.39)
133 (4.01)
140 (4.22)
211 (6.36)
14 (0.42)
47 (1.42)
61 (1.84)
13 (0.39)
98 (3.00)
494 (14.90)
347 (10.46)
*Median and interquartile range of age of positive cases for different pathogens.
The median age of patients with at least one positive pathogen was lower than that of patients who tested negative for any of etiologies [4 years (IQR 2–20) vs. 9 years (2 –29)] (P<0.001, Mann-Whitney test). Compared with patients who were detected with multiple etiologies, patients detected with single etiology were older [5 years (IQR 2 –26) vs. 3 years (IQR 2 –7)] (P<0.001, Mann-Whitney test). The median age of the patients with laboratory-confirmed Flu A, Flu B and HSV was considerably higher than that of patients with ADV, HRV, RSV, and hCoV-NL63 and hCoV-HKU1 (P<0.001, LSD test). The patients testing positive for H. influenzae were older than those positive for S.pneumoniae (P<0.001, Mann-Whitney test) (Table 1).
There was no pathogen-specific significant difference in the detection rate between male and female patients.
Etiologic distribution according to regions and years
Since specimens were collected from three cities located in the southern, central and northern parts of Jiangsu Province, the etiologic detection rate in ILI patients from three regions were compared. Flu A, Flu B, HRV and HSV were detected less commonly in Suzhou city (P<0.005), while RSV, hCoV-NL63, S. pneumoniae and H. influenzae were more frequently detected in Nanjing. Among these pathogens, only the detection rate of ADV showed no difference between different regions. At the same time, we compared the etiologic distribution in different years. Similar to the regional distribution, the prevalence of ADV was consistent across different years, while the remaining pathogens were different (Table 2).
Table
2.
Etiologies distribution in different regions and years
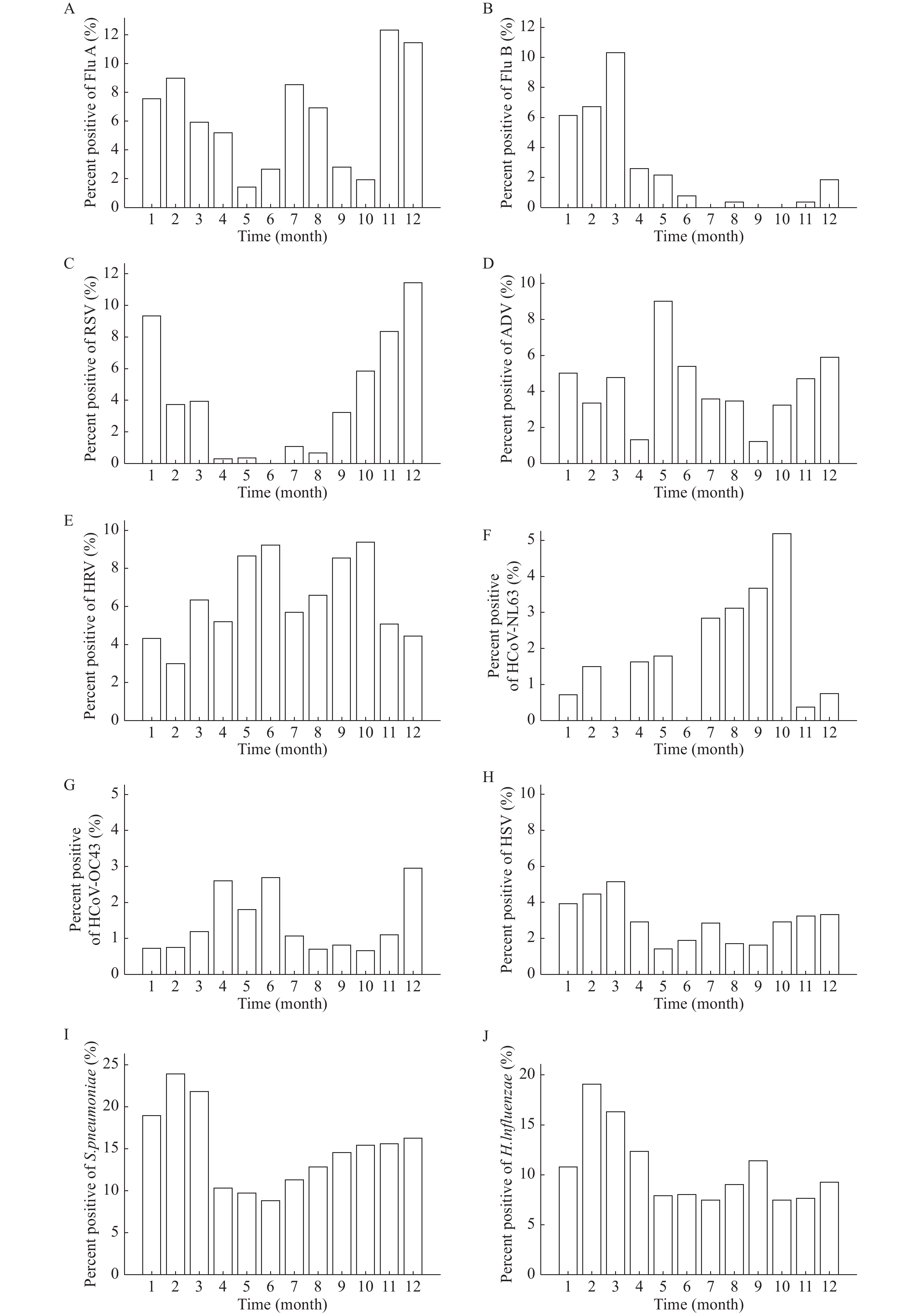
The detection rates of pathogens were not evenly distributed during different seasons over the 5-year period. Flu A, Flu B, RSV, HSV, and S. pneumoniae were detected most often during winter and spring.
However, Flu A also occurred in summer. ADV mainly occurred in May, although it was identified all year. There were no clear seasonal characteristics with HRV and H. influenzae, given that it was detected frequently all year. As for coronavirus, HCoV-OC43 was detected most frequently in spring while hCoV-NL63 was detected mostly in autumn (Fig. 1). Seasonal index was calculated monthly for the etiologies whose detection rate reached more than 2% (Table 3). Flu C, hCoV-HKU1 and hCoV-229E were detected in few samples, hence, their seasonal pattern could not be determined.
Table
3.
Seasonal index of pathogens with detection rate greater than 2%
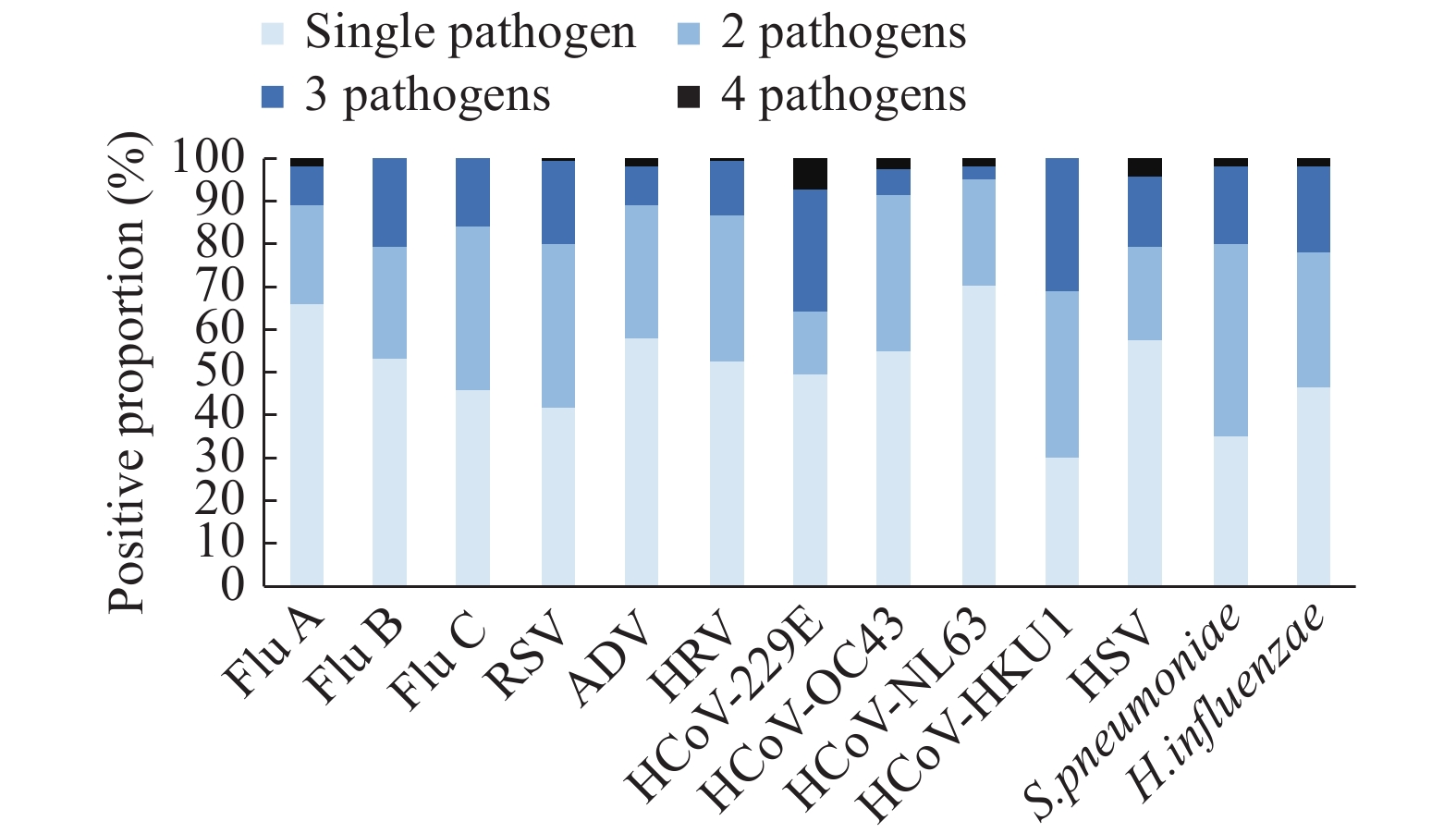
Among 3 316 patients with ILI, co-detection of multiple pathogens was found in 419 cases. Two pathogens were found in 315 patients, 3 pathogens in 97 patients, and 4 pathogens in 7 patients (Table 4, Fig. 2).
Table
4.
Positive proportion for single pathogen and multiple pathogens among 3 316 patients with ILI in Jiangsu province in 2012−2016 [n (%)]
Co-infections of S. pneumoniae with one or more viruses were detected in 260 patients, thereinto HRV (63 cases, 24.23%) and RSV (61 cases, 23.46%) were co-detected with it. Co-infections of H. influenzae with one or more virus were found in 125 cases, thereinto Flu A (30 cases, 24.00%) and HRV (27 cases, 21.60%) were co-detected with it. For those infected with 3 pathogens, S. pneumoniae, H. influenzae and a single virus were co-detected in 62 cases (63.92%). For those infected with 4 pathogens, S. pneumoniae, H. influenzae, FluA and HSV viruses were co-detected in 3 cases (42.86%) (Table 5 and Table 6).
Table
5.
The combining form of two pathogens among 3 316 patients with ILI in Jiangsu province in 2012–2016 (n)
ILI is a complex and diverse group of diseases. It is difficult to differentiate various pathogens by its symptoms, because different etiologic agents can cause similar symptoms. Some pathogens arise in outbreaks in schools or other locations[18–19]. These pathogens may lead to severe respiratory system infections that need intensive care therapy or can even lead to death[7, 20]. In this study, multiple respiratory pathogens were analyzed through nasopharyngeal swab samples that were collected over 5 years from three cities across Jiangsu province.
Flu A was one of the frequently isolated viruses in all cases of this study, which showed a seasonal distribution with high peaks in winter and summer. This pattern matches the known influenza epidemic pattern in southern China[21]. Our results also demonstrated that Flu A accounts for a large burden of disease in Jiangsu Province, and vaccination for influenza should be used widely, especially in children 6–9 years of age who are in nursery or primary school, and in those 50–64 years of age.
It is clear that HRV can cause pneumonia in people of any age[22–24]. It is also an important pathogen for co-infections. In this study, the HRV has been found to be an important agent on the spectrum of ILI etiology. However, the infection rate of HRV declined significantly with increasing age.
More than 90 genotypes of ADV are known to infect humans, accounting for 5%–10% of respiratory illnesses in children[25]. We found a seasonal variation in detection of ADV, peaking in May to July every year, which is different from other pathogens detected in our study. Furthermore, we found that the rate of ADV infection was higher in children 6 –9 years of age who are in nursing and primary school, surrounded by other children. ADV outbreaks have occurred in intensive care units, schools, and military camps, usually associated with crowded or closed environments[18– 19]. Thus, we speculate that ADV is one of the major causative agents associated with respiratory infection in students, especially in primary schools.
RSV is one of the most important respiratory pathogens among infants worldwide[26– 27]. It was one of the most frequently isolated viruses among children less than 5 years, especially in infants less than 6 months, in our study. Regarding the seasonality, the RSV epidemic peaked during winter as the season index was high in October to January. RSV can cause re-infections throughout life but most of adults show only mild respiratory infections without fever. So It is speculated that the infection rate of RSV will be higher in grown-up patients with acute respiratory infections showing no fever.
In our study, HSV was isolated from 98 (3.0%) ILI cases, 57 (58.16%) of which had no other virus detected. It is unusual that HSV was included in the study of respiratory infection in China, as it has not been widely studied previously. However, one report from South America obtained the similar result, in which HSV was isolated from 164 (2.6%) patients with ILI. Viral co-infection was detected in 34 (20.7%) HSV-positive cases[28]. However, HSV has been reported as a common agent resulting in viral pneumonia[29]. It should be noted that co-detection in HSV-positive cases was not higher than other pathogens in this study. Nevertheless, these data suggest that in the future, HSV should be considered in diagnosis as a potential cause of ILI.
S. pneumoniae and H. influenzae are common pathogens that can occur as non-infectious colonization in healthy people. Few studies have reported their carriage rates in patients with ILI in China. In our study S. pneumoniae was the most frequently detected pathogen with a positivity rate of 14.90%. Moreover, it was also the one most frequently identified in co-infection. Many factors contribute to the prevalence of S. pneumoniae and H. influenzae carriage, including age, season, geographical area, acceptance of vaccination, antibiotic consumption, sampling technique, and type of infant feeding[30]. The detection rate was a little low compared with other studies in health populations, which may be attributed to high antibiotic consumption during ILI onset[31].
Many reports have demonstrated that 2 or 3 viral species can be detected in 10%–20% of children with pneumonia, and that mixed viral-bacterial infection can be found in up to 45% of cases[16–17], which is consistent with the results of our study. Detection of multiple pathogens in a fairly high proportion of cases has been a feature in etiological studies of respiratory infection when PCR is used. We recognize that PCR-based methods are more sensitive than conventional diagnostic methods (culture, antigen detection, and serological assays)[32]. The most typical combination is S. pneumoniae with various respiratory viruses, especially with HRV. However, the interactions of agents in vivo is poorly understood to date, and these interactions may be complementary or inhibitory[33]. Subjects in our study were outpatients tested within 3 days of disease onset. Further observation could help in understanding the association between co-infection and disease severity.
There were a few limitations in our study. First, the patients with ILI who were enrolled in this study were outpatients within 3 days of disease onset. We did not follow them to investigate the progression of the disease; hence, it was not possible to know which pathogen led to severe clinical manifestations. Second, pathogens were not cultured in this study. A positive result following PCR only indicates pathogen carriage, but does not necessarily indicate that the agent is responsible for the ILI. Third, data for antibiotics and antiviral drug use were not collected; however, these factors may have confounded the results.
In summary, this study reports important information on the respiratory etiology in patient with ILI in Jiangsu province, eastern China. HRV, Flu A, and ADV were the main viruses identified in ILI patients. A high co-detection rate of S. pneumoniae, H. influenzae, and HRV was found in these patients. The distribution of the diverse etiologies varied by season, age and region. The spectrum of etiologies could help to estimate disease burden of the pathogens and provide robust evidence to guide vaccination programs. Further studies are needed to investigate the association between the etiology and disease severity.
Acknowledgments
We would like to thank doctors and nurses in six sentinel hospitals who participated in this program, the subjects and their guardians for participation in this study, and our colleagues, whose names were not listed as authors, for their assistance in data and samples collection. We would like to thank Editage for English language editing. This work was supported by the Jiangsu Provincial Major Science & Technology Demonstration Project (No. BE2017749), and the Jiangsu Province Science & Technology Demonstration Project for Emerging Infectious Diseases Control and Prevention (No. BE2015714).
Liu L, Johnson HL, Cousens S, et al. Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000[J]. Lancet, 2012, 379(9832): 2151–2161. doi: 10.1016/S0140-6736(12)60560-1
[2]
Mizgerd JP. Lung infection-A public health priority[J]. PLoS Med, 2006, 3(2): e76. doi: 10.1371/journal.pmed.0030076
Lekana-Douki SE, Nkoghe D, Drosten C, et al. Viral etiology and seasonality of influenza-like illness in Gabon, March 2010 to June 2011[J]. BMC Infect Dis, 2014, 14: 373. doi: 10.1186/1471-2334-14-373
[5]
Ye CC, Zhu WP, Yu JX, et al. Viral pathogens among elderly people with acute respiratory infections in Shanghai, China: preliminary results from a laboratory-based surveillance, 2012-2015[J]. J Med Virol, 2017, 89(10): 1700–1706. doi: 10.1002/jmv.24751
[6]
Stempel HE, Martin ET, Kuypers J, et al. Multiple viral respiratory pathogens in children with bronchiolitis[J]. Acta Paediatr, 2009, 98(1): 123–126. doi: 10.1111/j.1651-2227.2008.01023.x
[7]
Mistry RD, Fischer JB, Prasad PA, et al. Severe complications in influenza-like illnesses[J]. Pediatrics, 2014, 134(3): e684–e690. doi: 10.1542/peds.2014-0505
[8]
Prayle A, Atkinson M, Smyth A. Pneumonia in the developed world[J]. Paediatr Respir Rev, 2011, 12(1): 60–69. doi: 10.1016/j.prrv.2010.09.012
[9]
Huijskens EG, Biesmans RC, Buiting AG, et al. Diagnostic value of respiratory virus detection in symptomatic children using real-time PCR[J]. Virol J, 2012, 9: 276. doi: 10.1186/1743-422X-9-276
[10]
Kim JK, Jeon JS, Kim JW, et al. Epidemiology of respiratory viral infection using multiplex RT-PCR in Cheonan, Korea (2006-2010)[J]. J Microbiol Biotechnol, 2013, 23(2): 267–273. doi: 10.4014/jmb.1212.12050
[11]
Brunstein JD, Cline CL, McKinney S, et al. Evidence from multiplex molecular assays for complex multipathogen interactions in acute respiratory infections[J]. J Clin Microbiol, 2008, 46(1): 97–102. doi: 10.1128/JCM.01117-07
[12]
Jartti T, Jartti L, Ruuskanen O, et al. New respiratory viral infections[J]. Curr Opin Pulm Med, 2012, 18(3): 271–278. doi: 10.1097/MCP.0b013e328351f8d4
[13]
Van der Hoek L, Pyrc K, Jebbink MF, et al. Identification of a new human coronavirus[J]. Nat Med, 2004, 10(4): 368–373. doi: 10.1038/nm1024
[14]
Esper F, Weibel C, Ferguson D, et al. Evidence of a novel human coronavirus that is associated with respiratory tract disease in infants and young children[J]. J Infect Dis, 2005, 191(4): 492–498. doi: 10.1086/428138
[15]
Fouchier RAM, Hartwig NG, Bestebroer TM, et al. A previously undescribed coronavirus associated with respiratory disease in humans[J]. Proc Natl Acad Sci USA, 2004, 101(16): 6212–6216. doi: 10.1073/pnas.0400762101
[16]
Paranhos-Baccalà G, Komurian-Pradel F, Richard N, et al. Mixed respiratory virus infections[J]. J Clin Virol, 2008, 43(4): 407–410. doi: 10.1016/j.jcv.2008.08.010
[17]
Diaz J, Morales-Romero J, Pérez-Gil G, et al. Viral coinfection in acute respiratory infection in Mexican children treated by the emergency service: a cross-sectional study[J]. Ital J Pediatr, 2015, 41: 33. doi: 10.1186/s13052-015-0133-7
[18]
Centers for Disease control (CDC). Adenovirus type 7 outbreak in a pediatric chronic-care facility-Pennsylvania, 1982[J]. MMWR Morb Mortal Wkly Rep, 1983, 32(19): 258–260.
[19]
Sánchez MP, Erdman DD, Török TJ, et al. Outbreak of adenovirus 35 pneumonia among adult residents and staff of a chronic care psychiatric facility[J]. J Infect Dis, 1997, 176(3): 760–763. doi: 10.1086/517295
[20]
Rudan I, Boschi-Pinto C, Biloglav Z, et al. Epidemiology and etiology of childhood pneumonia[J]. Bull World Health Organ, 2008, 86(5): 408–416. doi: 10.2471/BLT.07.048769
Libster R, Bugna J, Coviello S, et al. Pediatric hospitalizations associated with 2009 pandemic influenza A (H1N1) in Argentina[J]. N Engl J Med, 2010, 362(1): 45–55. doi: 10.1056/NEJMoa0907673
[23]
Håberg SE, Trogstad L, Gunnes N, et al. Risk of fetal death after pandemic influenza virus infection or vaccination[J]. N Engl J Med, 2013, 368(4): 333–340. doi: 10.1056/NEJMoa1207210
[24]
Chen WJ, Arnold JC, Fairchok MP, et al. Epidemiologic, clinical, and virologic characteristics of human rhinovirus infection among otherwise healthy children and adults: rhinovirus among adults and children[J]. J Clin Virol, 2015, 64: 74–82. doi: 10.1016/j.jcv.2015.01.007
[25]
Chen HL, Chiou SS, Hsiao HP, et al. Respiratory adenoviral infections in children: a study of hospitalized cases in southern Taiwan in 2001-2002[J]. J Trop Pediatr, 2004, 50(5): 279–284. doi: 10.1093/tropej/50.5.279
[26]
Hall CB, Weinberg GA, Iwane MK, et al. The burden of respiratory syncytial virus infection in young children[J]. N Engl J Med, 2009, 360(6): 588–598. doi: 10.1056/NEJMoa0804877
[27]
Iwane MK, Edwards KM, Szilagyi PG, et al. Population-based surveillance for hospitalizations associated with respiratory syncytial virus, influenza virus, and parainfluenza viruses among young children[J]. Pediatrics, 2004, 113(6): 1758–1764. doi: 10.1542/peds.113.6.1758
[28]
Laguna-Torres VA, Gómez J, Ocaña V, et al. Influenza-like illness sentinel surveillance in Peru[J]. PLoS One, 2009, 4(7): e6118. doi: 10.1371/journal.pone.0006118
[29]
Ruuskanen O, Lahti E, Jennings L C, et al. Viral pneumonia[J]. Lancet, 2011, 377(9773): 1264–1275. doi: 10.1016/S0140-6736(10)61459-6
[30]
García-Rodríguez JA, Martínez MJF. Dynamics of nasopharyngeal colonization by potential respiratory pathogens[J]. J Antimicrob Chemother, 2002, 50 Suppl S2: 59–73.
[31]
Wang AH, Yu SJ, Yao KH, et al. Antimicrobial susceptibility of Haemophilus influenzae strains and antibiotics usage patterns in pediatric outpatients: results from a children's hospital in China (2000-2004)[J]. Pediatr Pulmonol, 2008, 43(5): 457–462. doi: 10.1002/ppul.20789
[32]
Murdoch DR, Jennings LC, Bhat N, et al. Emerging advances in rapid diagnostics of respiratory infections[J]. Infect Dis Clin North Am, 2010, 24(3): 791–807. doi: 10.1016/j.idc.2010.04.006
[33]
Canducci F, Debiaggi M, Sampaolo M, et al. Two-year prospective study of single infections and co-infections by respiratory syncytial virus and viruses identified recently in infants with acute respiratory disease[J]. J Med Virol, 2008, 80(4): 716–723. doi: 10.1002/jmv.21108
 Authors and Reviewers
Authors and Reviewers

 DownLoad:
DownLoad: